Few things test a new parent’s patience, resilience, and sanity quite like the relentless, high-pitched crying of a baby with colic. If you’re reading this in the wee hours of the morning, perhaps with a fussy infant cradled in your arms, know that you are not alone. Colic is an incredibly common, albeit distressing, phenomenon that affects countless families worldwide. It can turn the joyful, albeit exhausting, initial weeks of parenthood into a stressful period of confusion and exhaustion. But what exactly is colic? Is it a disease? Is your baby in pain? And, most importantly, when will it end and how can you soothe your little one? This comprehensive guide dives deep into everything you need to know about colic, from recognizing the diagnostic criteria to actionable, research-backed strategies for soothing your baby and, crucially, caring for yourself.
Understanding Colic: Beyond the Crying
Colic is not a diagnosis of a specific disease or an indication that your baby is unwell in the conventional sense. Instead, it’s a descriptive term used by pediatricians and researchers to define a pattern of excessive, frequent, and intense crying in an otherwise healthy and well-fed infant. The classic clinical definition of colic, often attributed to pediatrician Dr. Morris Wessel in the 1950s and famously known as the “Rule of Threes,” states that a baby has colic if they cry for:
- More than three hours a day,
- More than three days a week,
- For more than three consecutive weeks.
While this rule provides a useful baseline, modern pediatricians tend to view colic more broadly. Today, colic is often understood as a self-limiting behavioral syndrome characterized by paroxysmal (sudden onset) fussing, crying, or irritability, typically occurring in the first four months of life. It’s essential to emphasize the phrase “otherwise healthy.” This means before attributing excessive crying to colic, a pediatrician must rule out underlying medical issues such as infections, reflux, or milk protein allergies. It’s a diagnosis of exclusion.
The Prevalence of Colic
If you’re dealing with a colicky baby, you’re certainly in good company. Statistics estimate that colic affects anywhere from 10% to 40% of all infants worldwide. This frequency makes it one of the most common reasons parents seek medical advice during their baby’s first few months. Interestingly, research consistently shows that colic occurs equally among first-born and subsequently born children, and it affects breastfed and formula-fed infants at similar rates. There is also no evidence linking colic to gender, socioeconomic status, or gestational age at birth.
The Standard Timeline
The good news, which might seem distant when you’re living it, is that colic is temporary. It almost always follows a predictable timeline. Symptoms typically begin around the second or third week of life (or slightly later in pre-term infants), peak between six and eight weeks, and significantly subside by three to four months. By five or six months of age, colic symptoms have naturally resolved in the vast majority of cases. While this provides reassurance that there is an end in sight, understanding this timeline is also crucial for managing expectations and planning coping strategies for the weeks ahead.
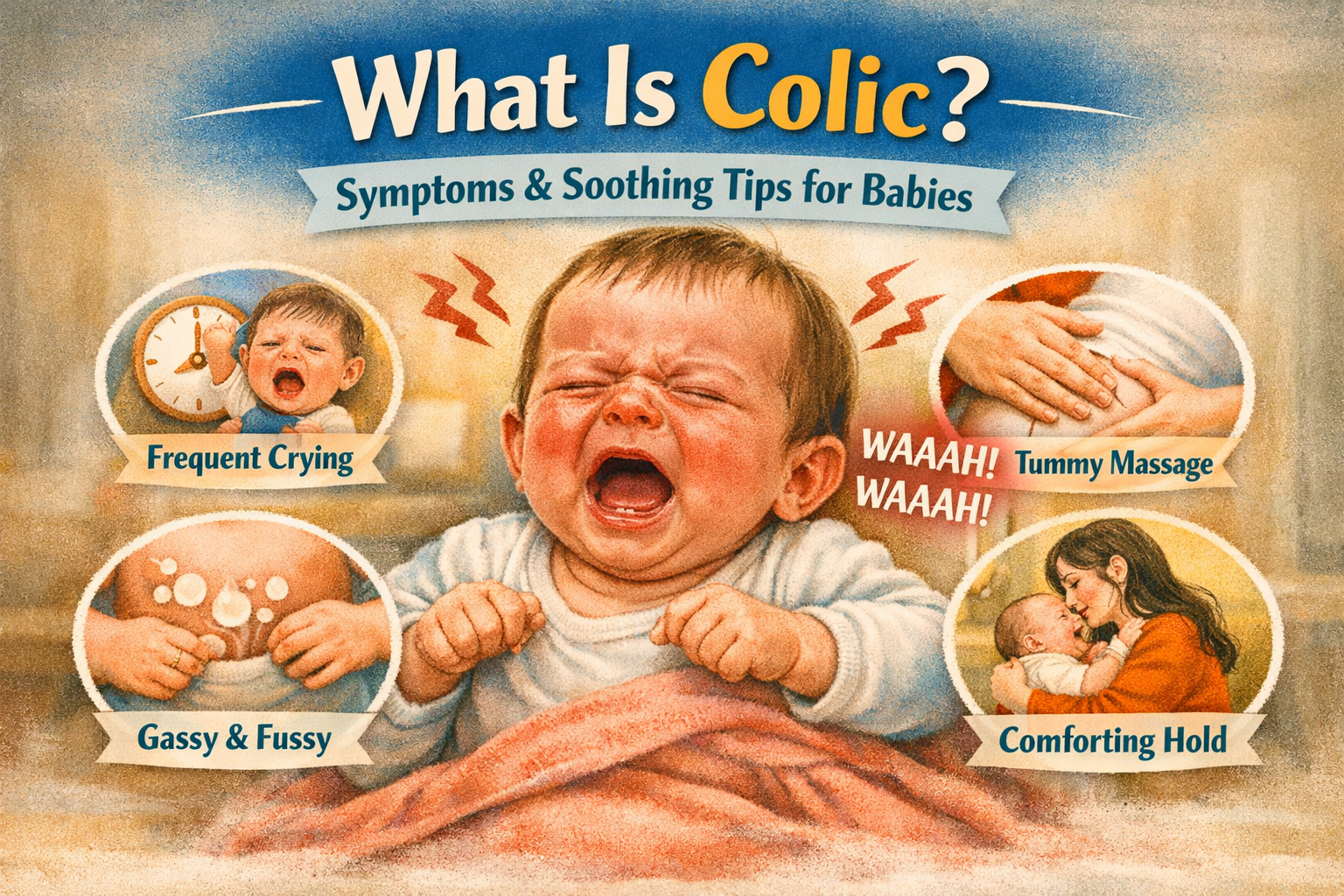
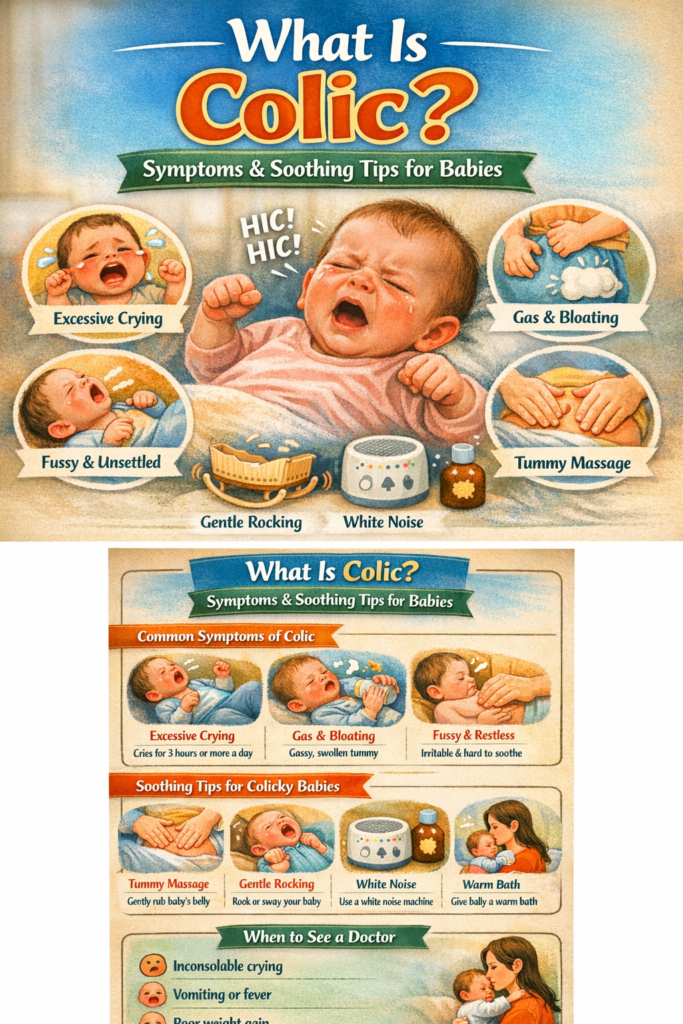
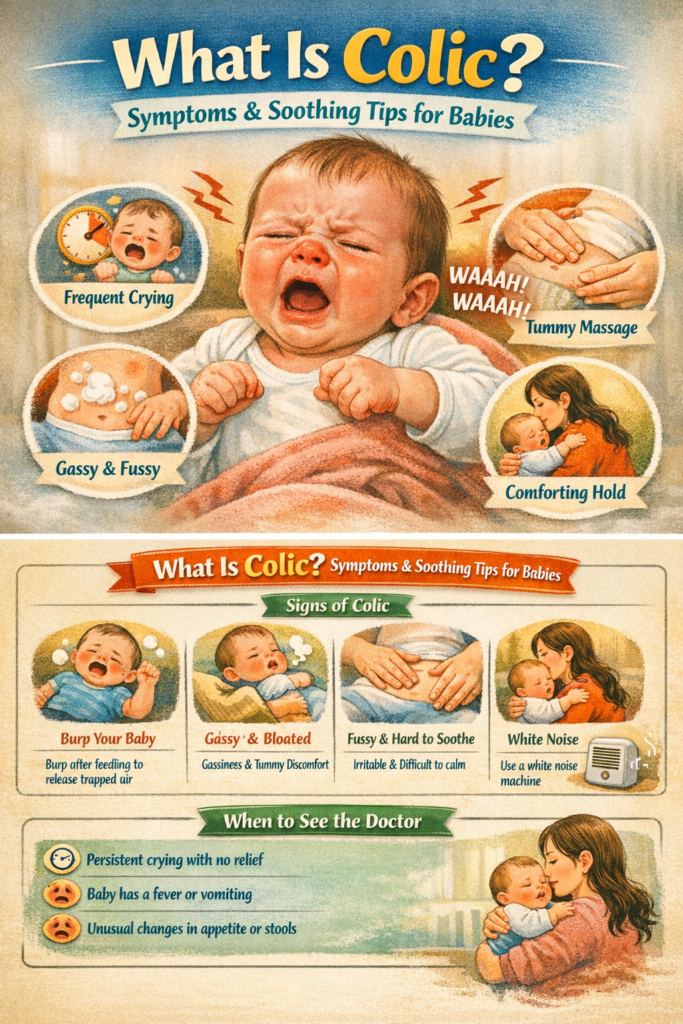
The Distinct Symptoms of Colic
Distinguishing colicky crying from normal infant fussiness—which is often triggered by hunger, a wet diaper, or fatigue—is key to identifying if your baby might be experiencing colic. Normal fussiness usually resolves once the underlying need is met. Colic, however, is often characterized by several distinct features:
1. Intense and Inconsolable Crying
The most defining symptom of colic is the quality and quantity of the crying. It’s not just fussing; it’s often described as a loud, high-pitched, almost piercing scream. The baby seems conceptually distressed and uncomfortable. Unlike normal crying, which might have varied intonations, colicky crying often sounds unrelenting and sometimes urgent. The most frustrating aspect for parents is that this crying is frequently inconsolable. You might feed, burp, change, and rock your baby, but the intense crying continues seemingly unabated, often lasting for several hours at a time. This pattern typically emerges in the late afternoon or evening, which exhausted parents often refer to as the “witching hour(s).”
2. Specific Postural Changes
When a baby is experiencing a colicky episode, their physical behavior often shifts. They don’t just cry; they physically react, appearing as if they are in discomfort, which can be distressing to witness. These postural changes are a key indicator:
- Clenched Fists: During intense crying fits, babies with colic often tightly clench their fists. This is a common physical sign of overall distress and tension.
- Arched Back: You may notice your baby arching their back stiffly. While this can sometimes be associated with reflux (which needs to be ruled out by a doctor), in the context of colic, it often represents a total-body reaction to distress or gas.
- Tense Abdomen and Curled Legs: The baby’s belly might feel hard or tight to the touch. Simultaneously, they frequently pull their legs up towards their chest, which is a classic posture associated with abdominal pain or gas. While these postural changes make it seem like the baby has stomach pain, the exact cause remains debated.
- Flushed Face: The sheer intensity of the crying often causes the baby’s face to become extremely red or flushed, adding to the appearance of intense distress.
3. Gas and Abdominal Distension
Many parents of colicky babies observe that their infants pass a lot of gas or appear bloated. It’s a “chicken and egg” scenario: is the baby crying because of trapped gas, or are they swallowing excessive air because they are crying so intensely? In reality, it’s often a combination of both. When a baby cries vigorously for hours, they inevitably swallow significant amounts of air, which can then lead to further abdominal discomfort and distension, creating a self-perpetuating cycle of crying and gas. While passing gas may seem to offer temporary relief, the underlying colicky pattern usually continues.
It’s important to reiterate that while these symptoms are characteristic of colic, you should always consult your pediatrician if you are concerned about your baby’s crying patterns. A doctor needs to confirm that your baby is gaining weight normally and that there are no underlying medical conditions contributing to the distress, such as gastroesophageal reflux disease (GERD), an undiagnosed infection, or an allergy to cow’s milk protein found in formula or breast milk.
Potential Causes and Theories: Why Does Colic Happen?
Perhaps the most frustrating aspect of colic for both parents and medical professionals is that we still don’t know its exact cause. It is widely considered a multi-factorial condition, meaning several different factors likely contribute to its development. Over the years, numerous theories have emerged, and while none are universally proven, they offer insight into the complexities of the syndrome:
The Immature Digestive System Theory
This is one of the most prominent theories. It suggests that colic is related to a baby’s developing digestive system. Proponents argue that a newborn’s gut is still learning how to process food and move waste efficiently. This immaturity might lead to:
- Intestinal Hypermotility: The muscles in the intestines might spasm or contract too vigorously (hypermotility), causing pain similar to cramping.
- Gas Imbalance: The complex microbiome—the community of bacteria in the gut—is still establishing itself. An imbalance or “dysbiosis” in this microbiome might lead to increased gas production and subsequent discomfort. Some research has shown differences in the gut bacteria of colicky babies compared to non-colicky babies.
- Temporary Lactose Intolerance: Some researchers have hypothesized a temporary, functional lactase deficiency. Lactase is the enzyme needed to digest lactose, the sugar found in breast milk and formula. If a baby isn’t producing enough lactase, undigested lactose can ferment in the gut, leading to significant gas and bloating.
The Immature Nervous System and Overstimulation Theory
Another compelling theory focuses on the baby’s developing nervous system and their inability to regulate their response to stimuli. This perspective views colic as a result of:
- Sensory Overload: Newborns enter a world filled with lights, sounds, and sensations they’ve never experienced. Some babies may be more sensitive to this sensory input and, by the end of the day, their immature nervous system becomes overloaded and unable to self-soothe. They might continue to cry simply because they can’t “tune out” the world or settle themselves.
- Inability to Regulate: These babies might lack the developmental ability to shift from an alert or agitated state back to a calm state, essentially getting “stuck” in a cycle of crying.
The Behavioral and Parent-Infant Interaction Theory
Historically, it was sometimes suggested that colic was linked to maternal anxiety or poor parenting techniques. However, this theory has been widely discredited. Modern research consistently shows that colic occurs equally among infants with parents of all temperaments and experience levels. While parental stress is certainly an outcome of managing a colicky baby, there is no credible evidence suggesting that anxiety or “wrong” parenting causes the condition.
Migraine Precursor Theory
A newer and intriguing theory suggests a potential link between infantile colic and a predisposition to childhood migraines. This hypothesis posits that colic might be an early manifestation of a migraine-like condition in infants, who may be experiencing sensory overload (such as light or sound sensitivity) that is later expressed as migraines. More research is needed in this area, but it suggests a neurological, rather than strictly gastrointestinal, root for some cases of colic.
Effective Soothing Tips for Colicky Babies
When your baby is in the midst of a colicky episode, your immediate priority is comfort and soothing. Because the exact cause is often unclear, the best approach is to systematically try different techniques to see what works for your unique baby. What soothes your baby one day might not work the next, so patience and a willingness to rotate through strategies are essential. Here are some of the most effective, research-backed, and expert-recommended soothing tips:
The “5 S’s” Strategy
Developed by pediatrician Dr. Harvey Karp, the “5 S’s” approach aims to trigger a baby’s “calming reflex” by mimicking the environment of the womb. Many parents find this sequence highly effective:
- Swaddle: Snug swaddling keeps a baby’s arms from flailing (which can startle them) and provides a sense of security similar to being in the womb. Ensure the swaddle is secure but not so tight that it restricts hip movement.
- Side or Stomach Position: While babies must always sleep on their backs to reduce the risk of SIDS, the side or stomach position (while being held) can be very soothing when they are awake and fussy. Try holding your baby on their side or stomach in your arms while gently supporting their head.
- Shush: Newborns are used to the loud, constant “whooshing” sound of blood flow in the womb, which is louder than a vacuum cleaner. Mimic this with rhythmic, loud (but not damagingly so) “shushing” near their ear. A white noise machine or even a fan can also be effective.
- Swing: Rhythmic motion is incredibly calming. While swinging your arms can be tiring, using a safe baby swing or taking a car ride can provide the necessary movement. Gentle, rhythmic bouncing on a therapy ball while holding the baby also works well.
- Suck: Sucking is a natural self-soothing mechanism for babies. Offer a pacifier or your clean finger (or allow them to breastfeed for comfort, even if they aren’t hungry) to help them calm down.
Nutritional and Dietary Adjustments
Given the gastrointestinal theories of colic, adjusting the baby’s intake (or the mother’s, if breastfeeding) is often one of the first avenues parents explore. These changes should always be made under the guidance of a pediatrician:
For Breastfed Infants:
- Maternal Elimination Diet: Some research suggests that elimination of certain allergenic foods from the mother’s diet can reduce colic symptoms in some breastfed infants. Common culprits include cow’s milk, eggs, peanuts, tree nuts, wheat, soy, and fish. This approach requires strict adherence and should be discussed with a doctor or dietitian to ensure maternal nutrition isn’t compromised.
- Manage Fore-milk/Hind-milk Imbalance: If a mother has an overabundant milk supply, the baby might be receiving too much of the lactose-rich “fore-milk” and not enough of the fattier “hind-milk.” This high lactose load can ferment in the gut, causing gas. Ensuring the baby finishes one breast completely before switching to the other can help balance this.
For Formula-Fed Infants:
- Switch Formula: If a pediatrician suspects a cow’s milk protein allergy or sensitivity (which is distinct from colic but can cause similar symptoms), they may recommend switching to a hypoallergenic formula. These formulas contain protein that is extensively broken down (hydrolyzed), making it easier to digest and less likely to trigger an allergic response. Partially hydrolyzed formulas are sometimes tried first, although the evidence for their effectiveness in true colic is less robust.
Supplements:
- Probiotics: Research into probiotics, particularly the strain Lactobacillus reuteri (DSM 17938), has shown promise. Several studies indicate that supplementation with L. reuteri can significantly reduce crying time in some (primarily breastfed) colicky infants. Probiotics work by helping to balance the baby’s gut microbiome.
- Lactase Drops: For cases suspected to involve temporary lactose intolerance, lactase enzyme drops (such as Colief) can be added to breast milk or formula. These drops help break down the lactose before feeding, potentially reducing gas and bloating. The effectiveness of lactase drops for colic is still debated in the medical community, but they are generally considered safe to try.
For a deeper dive into the world of overall baby care beyond colic, exploring a comprehensive collection of essential baby products can provide insights into creating a comfortable and nurturing environment for your little one.
Movement, Touch, and Environmental Changes
Sometimes, the simplest approach—changing the sensory input—is the most effective. These strategies often work by providing a new focal point or by directly soothing physical tension:
- The “Colic Carry”: This specialized hold often provides relief. Lay your baby chest-down on your forearm, supporting their head in your hand. Use your other hand to gently pat or rub their back. The gentle pressure on their abdomen can help relieve gas discomfort, and the close contact is comforting.
- Baby Massage: A gentle massage can relax the baby’s muscles and help move gas through the system. Focus on the tummy, using clockwise, circular motions and gently cycling the baby’s legs in a “bicycle” motion. Always ensure the baby is comfortable with touch; if they arch or seem more distressed, stop the massage.
- Warm Bath: A warm bath can be profoundly relaxing for some colicky babies, mimicking the warm, buoyant environment of the womb. However, other babies may find the change stimulating, so observe your baby’s reaction.
- Reduce Stimulation: If overstimulation is a factor, try the opposite of the “5 S’s.” Dim the lights, eliminate loud noises, and create a calm, quiet, and cool environment to help your baby’s nervous system downregulate.
- Get Outside: A change of scenery can sometimes work wonders. The combination of fresh air, natural light (even in the evening), and the gentle motion of a stroller walk can interrupt a crying cycle for both the baby and the parent.
A Comparative Look at Potential Remedies for Colic
When exploring options to soothe your colicky baby, it’s helpful to understand the level of scientific evidence supporting different approaches. While “what works for you” is ultimately the most important metric, knowing the general consensus can help you prioritize where to focus your efforts.
The following table provides a comparison of common colic remedies, summarizing their primary purpose and the scientific backing behind them:
| Remedy/Strategy | Primary Intended Purpose | Common Dosage/Use | Level of Scientific Evidence for Colic Relief | Key Considerations |
| Probiotics (L. reuteri) | Balance gut microbiome to reduce gas and inflammation. | Drops; often 5 drops daily. | Moderate-High (mostly breastfed) | Strongest evidence is for breastfed babies; consult a pediatrician for appropriate strain and dose. |
| Maternal Elimination Diet | Remove potential food allergens from breast milk. | Mother eliminates dairy, soy, eggs, etc. | Low-Moderate | Requires strict compliance and pediatrician/dietitian guidance to avoid nutritional deficiencies. |
| Hydrolyzed Formula | Provide easier-to-digest protein for infants with potential milk protein allergy/sensitivity. | Exclusive feeding of specialized formula. | Moderate (if allergy is suspected) | Not recommended unless milk protein allergy or severe sensitivity is strongly suspected by a pediatrician. |
| Gripe Water | Historically used for digestive upset (often contains herbs like fennel, ginger, chamomile). | Drops; given as needed. | Very Low | Scientific evidence is minimal; many brands exist, and ingredients vary. Look for alcohol-free and sugar-free versions, and always consult a pediatrician first. |
| Lactase Drops | Break down lactose in breast milk or formula to reduce gas/bloating. | Drops added to milk before feeding. | Low-Moderate | Evidence is mixed; generally considered safe to try but effectiveness is questionable. |
| Gas Drops (Simethicone) | Break up gas bubbles in the stomach. | Drops; given after or during feeds. | Very Low | Studies consistently show simethicone is no more effective than a placebo for colic. It is considered very safe, but likely won’t help colic. |
| The “5 S’s” Strategy | Trigger the calming reflex by mimicking the womb environment. | Sequential application of 5 soothing techniques. | Based on pediatric expertise/behavioral theory | While not backed by clinical trials specifically for colic diagnosis, it is highly recommended by many pediatricians and parents as an effective, safe soothing technique. |
| Baby Massage | Relax muscles, soothe, and promote digestion/gas passage. | Gentle tummy and body massage. | Low | Some small studies show benefits, but evidence is limited. It is a safe, bonding activity that may offer comfort. |
Coping as a Parent: Caring for Yourself During the Colic Phase
Living with a baby who has colic is undeniably challenging. The relentless crying, the lack of sleep, and the feeling of helplessness can take a significant toll on a parent’s mental and physical well-being. It is crucial to recognize that your exhaustion, frustration, and even anger are valid. Managing a colicky baby is one of the most stressful aspects of early parenthood, and prioritizing your self-care isn’t a luxury; it’s a necessity for navigating this difficult, yet temporary, season.
Managing Stress and Overwhelm
- Accept Help: This is not the time to be a hero. When friends or family offer to help, say yes. Let someone else hold the crying baby for an hour while you take a shower, nap, or simply sit in silence.
- Share the Load: If you have a partner, it’s essential to approach colic as a team effort. Rotate shifts during the high-fussiness periods. Knowing that you will have a guaranteed break can make the crying episodes more endurable.
- Take “Sanity Breaks”: It is perfectly okay—and sometimes necessary—to put your crying baby down in a safe place, like their crib, for 10-15 minutes. Walk into another room, close the door, practice deep breathing, and compose yourself. Taking a short break to regulate your own emotions is better than continuing to hold the baby while you are completely overwhelmed. As long as your baby is in a safe sleeping environment, a short period of crying will not harm them, and a calmer parent is better equipped to offer comfort.
- Connect with Others: Talking to other parents who have “been there” can provide immense comfort and validation. Knowing that your experience is common can alleviate feelings of isolation and failure. Online forums or local parenting groups are excellent resources.
When to Seek Immediate Help
The intense stress of caring for a colicky baby can contribute to postpartum depression or anxiety. It is essential to be aware of the signs and to seek help immediately if you experience:
- Feelings of intense sadness or hopelessness.
- Difficulty bonding with your baby.
- Severe anxiety or panic attacks.
- Thoughts of harming yourself or your baby.
If you are struggling, please reach out to your partner, your doctor, or a mental health professional. There is help available, and you do not have to go through this alone. Remember, caring for yourself is an integral part of caring for your baby.
In summary, colic is a difficult and temporary phase. While there is no single “cure,” understanding the symptoms, trying different soothing strategies, and prioritizing your own well-being can help you navigate this challenging time. For more general information on navigating the early stages of parenthood and finding community support, remember that you are part of a broader journey shared by many.
This challenging phase will pass. Until it does, rely on your pediatrician for support, prioritize your own sanity, and know that your love and care, even in the midst of the storm, make all the difference for your baby. You are not alone, and you will get through this.
Frequently Asked Questions
Understanding colic can be a confusing journey for new parents. Here are some of the most frequently asked questions, based on common Google “People Also Ask” intent, designed to provide direct and helpful answers.
What is the primary difference between a “fussy baby” and a “colicky baby”?
The primary difference lies in the predictability, intensity, and duration of the crying. All babies have fussy periods, which usually occur in response to a clear need like hunger, a dirty diaper, or fatigue, and are resolved when that need is met. Colic is defined by a specific, intense, and often inconsolable crying pattern—often summarized as crying for more than three hours a day, more than three days a week, for more than three weeks—in an otherwise healthy, well-fed infant. The crying episodes often start and stop without a clear reason and occur consistently, frequently in the evening.
At what age does colic typically begin, and when does it usually end?
Colic typically begins in the first two to three weeks of life (though it may be slightly later for pre-term infants). The crying episodes usually peak between six and eight weeks of age. The good news is that colic is almost always temporary. Symptoms significantly diminish by three to four months of age and have completely resolved for the vast majority of babies by five or six months.
Are breastfed babies less likely to have colic than formula-fed babies?
No. Research consistently shows that colic occurs at the same rate in breastfed babies as it does in formula-fed babies. While digestive issues or cow’s milk protein sensitivities (which can occur in both populations) are sometimes confused with colic, the specific syndrome of excessive, inconsolable crying affects infants equally regardless of how they are fed.
Is my baby in pain when they have colic?
This is one of the most distressing questions for parents. Because babies often clench their fists, arch their backs, and pull their legs up during a colic episode, it certainly looks like they are in pain, likely abdominal pain or gas. However, the exact cause of colic is unknown, and it’s not clear if they are actually experiencing pain. Some theories suggest colic may be related to an immature digestive or nervous system rather than direct pain, making them oversensitive to stimuli they can’t yet regulate. Crucially, colic is not linked to any long-term health problems.
Should I change my baby’s formula if they seem to have colic?
You should not change your baby’s formula without consulting your pediatrician. While switching to a hypoallergenic (extensively hydrolyzed) formula may help infants with a specific cow’s milk protein allergy or sensitivity (which a doctor must diagnose and which can cause symptoms similar to colic), it is generally not recommended as a first-line treatment for colic itself unless other symptoms (like eczema, blood in the stool, or failure to thrive) are present. Your doctor can help determine if a formula change is appropriate.
Can probiotics truly cure colic?
There is no definitive “cure” for colic. However, some research suggests that the specific probiotic strain Lactobacillus reuteri (DSM 17938) can significantly reduce the duration of crying in some infants with colic, particularly those who are exclusively breastfed. The results have been less conclusive for formula-fed babies. Probiotics are generally considered safe, but you should always discuss any supplement, including strain and dosage, with your pediatrician before giving it to your baby.
What are the most reliable soothing techniques for a baby with colic?
Because the cause of colic varies (or is unknown), the most reliable approach is often to try a combination of techniques, such as the “5 S’s” Strategy (Swaddle, Side/Stomach hold, Shush, Swing, Suck). Other effective methods include the “Colic Carry” (holding the baby tummy-down on your forearm), gentle baby massage, a warm bath, rhythmic motion (like a car ride or stroller walk), reducing environmental stimulation, and, if recommended by a pediatrician, nutritional adjustments such as probiotics or maternal dietary changes. It often requires patience and experimentation to find what works best for your baby.




