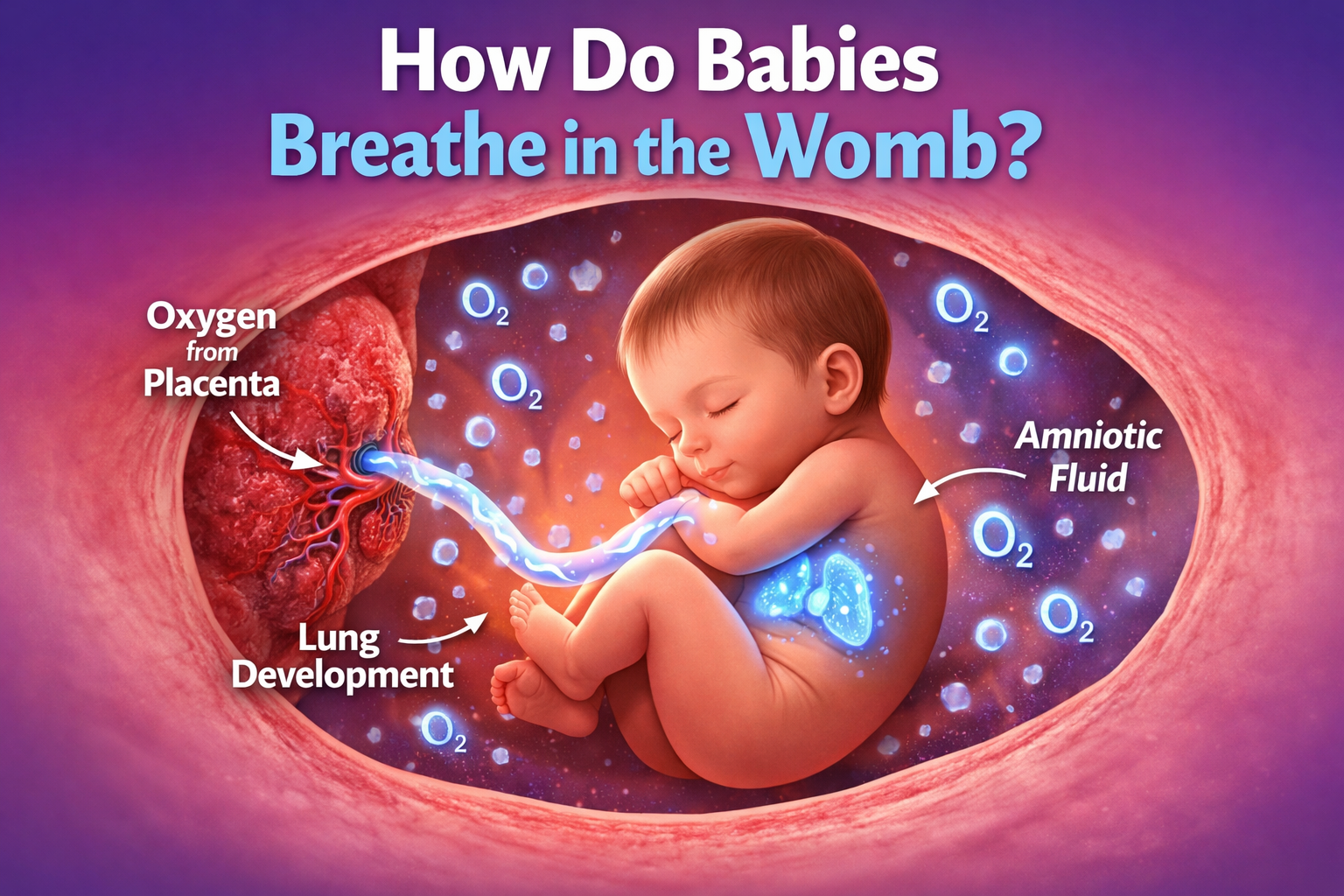
Babies do not breathe air in the womb. Instead, they receive all their necessary oxygen entirely through the mother’s bloodstream. The mother breathes in oxygen, which travels to the placenta and is delivered directly into the baby’s circulatory system via the umbilical cord. While developing fetuses make rhythmic “practice” breathing movements by swallowing amniotic fluid, their lungs do not process actual oxygen until their very first physical cry after birth.

The Biological Lifeline: The Placenta and Umbilical Cord
When you watch a pregnant woman breathe, she is quite literally breathing for two. The process of delivering oxygen to a fetus submerged in fluid is one of the most remarkable engineering feats in human biology. Because the amniotic sac is filled with fluid, traditional respiration—exchanging oxygen and carbon dioxide via lung tissue—is impossible. The body completely bypasses the lungs and relies on a dedicated, temporary organ: the placenta.
The placenta develops in the uterus during pregnancy, attaching to the uterine wall. It acts as the ultimate filtration and exchange system. When a mother inhales, oxygen enters her lungs, passes into her bloodstream, and travels to the placenta.
Here is where the magic happens. The mother’s blood and the baby’s blood never actually mix. Instead, they flow through a network of microscopic capillaries that sit so close to each other that oxygen, nutrients, and antibodies can easily pass through the membrane from the mother’s side to the baby’s side. Simultaneously, waste products like carbon dioxide transfer from the baby’s blood back into the mother’s blood, which she then exhales.
This highly oxygenated blood travels from the placenta to the baby through the umbilical cord. The umbilical cord contains three vital blood vessels:
- One large vein: This carries the nutrient-rich, oxygenated blood directly to the baby’s heart.
- Two smaller arteries: These carry the deoxygenated blood and waste products back to the placenta to be cleared by the mother’s body.
The Secret Weapon: Fetal Hemoglobin
You might wonder how a baby gets enough oxygen through this indirect delivery method. After all, by the time the oxygen reaches the baby, the mother’s body has already used a portion of it. The oxygen tension in fetal blood is surprisingly low—equivalent to an adult standing at the top of Mount Everest.
Fetuses survive and thrive in this low-oxygen environment because of a specialized protein called Fetal Hemoglobin (HbF).
Red blood cells contain hemoglobin, the molecule responsible for binding and carrying oxygen. Fetal hemoglobin is structurally different from adult hemoglobin. It has a significantly higher affinity for oxygen, meaning it can grab onto oxygen molecules much more tightly and efficiently than the mother’s blood cells can. Because of this powerful magnetic pull, the baby’s blood aggressively extracts the oxygen it needs as it passes through the placenta. By the time a baby reaches six months of age outside the womb, this specialized fetal hemoglobin is almost entirely replaced by standard adult hemoglobin.
As you spend your pregnancy researching these incredible biological milestones and shopping for your favorite newborn clothing and daily essentials, it is comforting to know that your body is naturally handling the complex heavy lifting of sustaining your child’s growth.
“Practice Breathing” in the Amniotic Sac
Even though babies do not use their lungs to process oxygen, they are not completely idle. Around week 10 to 12 of pregnancy, fetuses begin exhibiting what doctors call Fetal Breathing Movements (FBM).
During an ultrasound, you might actually see your baby’s chest rising and falling rhythmically. They are inhaling and exhaling amniotic fluid. This is a critical developmental milestone for several reasons:
- Muscle Development: Just like an athlete training for a marathon, the baby needs to build up the strength of their diaphragm and intercostal muscles (the muscles between the ribs). Swallowing and expelling the thick amniotic fluid provides heavy resistance training for these tiny muscles.
- Lung Expansion: The physical act of drawing fluid into the lungs forces the air sacs (alveoli) to stretch and grow. Without this fluid expansion, the lungs would remain permanently collapsed and underdeveloped.
- Surfactant Production: As the pregnancy progresses, particularly in the third trimester, the practice breathing helps distribute a crucial substance called surfactant. Surfactant is a slippery, soap-like coating that lines the inside of the lungs. It reduces surface tension, preventing the tiny air sacs from sticking together when the baby takes their first real breath of air.
If a baby is born prematurely, their primary medical challenge is often a lack of naturally produced surfactant. Modern medicine addresses this by administering synthetic surfactant, drastically improving the survival rates of premature infants.
Fetal Circulation: Bypassing the Lungs
Because the lungs are filled with fluid and not providing oxygen, sending a massive supply of blood to them would be a waste of the body’s energy. Fetal anatomy accounts for this with a highly specialized circulatory system that temporarily bypasses the lungs.
In a fetus, blood is rerouted using two temporary anatomical shortcuts:
- The Foramen Ovale: A small hole located between the upper two chambers (atria) of the heart. This allows highly oxygenated blood from the umbilical vein to move directly from the right side of the heart to the left side, completely skipping the trip to the lungs.
- The Ductus Arteriosus: A blood vessel connecting the pulmonary artery directly to the aorta. Any blood that does happen to pump toward the lungs is quickly diverted into the general circulation to feed the brain and organs.
Within minutes of a baby taking their first breath, the change in pressure causes these shunts to snap shut, fundamentally and permanently changing how their blood flows.
Fetal Oxygenation vs. Neonatal Breathing
Understanding the drastic shift between life inside and outside the womb highlights just how extreme the birth transition really is.
| Parameter | Inside the Womb (Fetal Stage) | After Birth (Neonatal Stage) |
| Primary Oxygen Source | The mother’s bloodstream via the placenta. | The surrounding atmospheric air. |
| Lung Status | Filled with amniotic fluid; inactive for gas exchange. | Filled with air; actively expanding and contracting. |
| Heart Routing | Blood bypasses the lungs via the foramen ovale and ductus arteriosus. | Shunts close; all blood routes through the lungs for oxygenation. |
| Breathing Trigger | Rhythmic practice driven by brain stem development. | Triggered by sudden temperature change, physical touch, and a spike in carbon dioxide. |
| Hemoglobin Type | Fetal Hemoglobin (HbF) – grabs oxygen aggressively. | Transitions rapidly to Adult Hemoglobin (HbA). |
The Big Transition: The First Real Breath
The moment of birth requires the most dramatic physiological shift a human being will ever experience. The transition from fluid-filled lungs to air-filled lungs happens in a matter of seconds.
As the baby is squeezed through the birth canal, the physical compression of their chest forcibly expels a large portion of the amniotic fluid from their lungs. This mechanical squeeze is highly beneficial. (Babies born via Cesarean section miss this “vaginal squeeze” and sometimes require a bit of extra help suctioning fluid from their airways).
Once the baby emerges, a combination of drastic changes triggers the respiratory center in their brain:
- Temperature Shock: Moving from a cozy 98.6-degree fluid environment to a cold, dry delivery room shocks the nervous system.
- Sensory Input: The sudden bright lights, loud noises, and physical handling stimulate the brain.
- Chemical Changes: When the umbilical cord is clamped, the baby’s carbon dioxide levels rapidly spike, and their oxygen levels drop. This chemical shift sends a frantic, urgent signal to the brain stem: Breathe now.
The baby gasps. As they take that massive first inhalation, the surrounding air rushes in, pushing the remaining amniotic fluid deep into the lung tissue where it is rapidly absorbed into the bloodstream. The physical expansion of the lungs changes the pressure in the chest cavity, forcing the fetal heart shunts to slam shut. The baby cries out, officially beginning their independent life.
While you are preparing your home and sourcing the safest, most comforting baby gear and nursery items to welcome your little one, your baby is busy inside the womb, tirelessly practicing the exact muscle movements they will need to greet you on delivery day. Finding reliable information on platforms like Wobblebee ensures you understand exactly what to expect during these incredible stages of early human development.
Frequently Asked Questions
Do babies drown in amniotic fluid?
No, babies cannot drown in the womb. Drowning occurs when lungs meant to process oxygen are flooded with water, cutting off the oxygen supply. Because a fetus receives 100% of its oxygen directly through the umbilical cord, the amniotic fluid in their lungs is totally safe and actually necessary for proper respiratory development.
When do a baby’s lungs fully develop?
While lungs begin forming early in the first trimester, they are one of the last major organs to reach full maturity. A baby’s lungs are generally considered fully functional and capable of independent breathing around week 36 of pregnancy.
Can a baby breathe if the umbilical cord is wrapped around its neck?
Yes, usually. A nuchal cord (umbilical cord wrapped around the neck) is quite common and happens in about 20% to 30% of pregnancies. Because the baby is not breathing through their windpipe, the cord resting on their neck does not choke them. The real danger only arises if the cord is pulled so tight that it cuts off the blood flow through the cord itself.
What happens when a baby takes its first breath?
The first breath triggers a massive chain reaction. The influx of air pushes the remaining fluid out of the lungs, decreases the resistance in the pulmonary blood vessels, and causes the temporary holes in the fetal heart to physically close. This forces the blood to begin circulating through the lungs to pick up oxygen.
Do babies practice crying in the womb?
Yes, ultrasound technology has captured fetuses displaying crying behaviors as early as the third trimester. They exhibit the same facial expressions, jaw tremors, and erratic swallowing patterns associated with crying, though they cannot make a sound because there is no air passing over their vocal cords.




